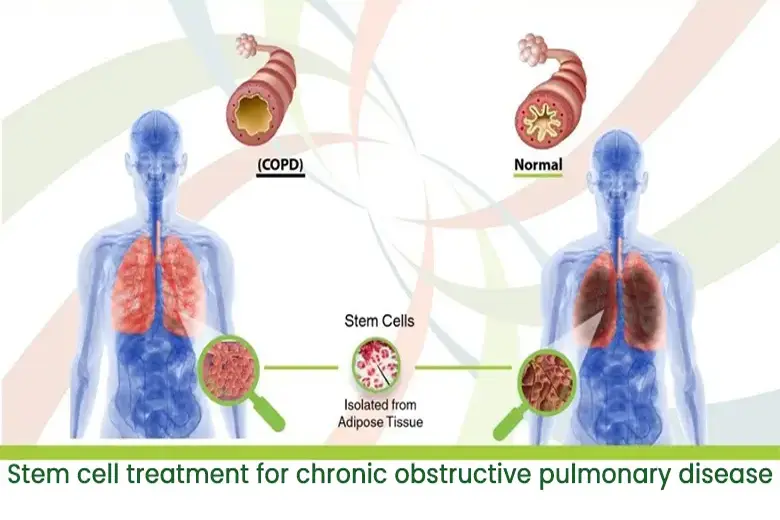
Chronic obstructive pulmonary diseaseis a major inflammatory disease of the airways and an enormous therapeutic challenge. Within the spectrum of chronic obstructive pulmonary disease, pulmonary emphysema is characterized by the destruction of the alveolar walls with an increase in the air spaces distal to the terminal bronchioles but without significant pulmonary fibrosis.
Idiopathic pulmonary fibrosis (IPF)is a chronic lung disease characterized by thickening and fibrosis of the alveolar walls. The etiology and pathogenesis are as yet unknown.
It is due to a response to some irritants, such as cigarette smoke, gastro-esophageal reflux and environmental pollution.
How It Is Done
Though the patho-physiology in both the diseases is different, however the treatment protocol remains the same.
Stem cells administered intravenously accumulate in interstitial and cells administered viaspecial nebulizer apparatusreach deep into alveoli. After intravenous infusion, maximum number of cells reach lungs, hence an effective therapeutic effect.
The cells provide Protection by differentiation of engrafted into specific and distinct lung cell phenotypes and triggering production of growth factors which mobilizes endogenous stem cells and with a decrease in inflammatory cytokine. Protection from fibrosis also involves suppression of inflammation.
What To Expect
In 80 % of patients, respiratory and forced volume capacity increases significantly, with FVC > 60% diffuse lung capacity for carbon monoxide-DLCO > 45% of the predicted values.
Breathing improves over time. Oxygen saturation improves and dependence on oxygen reduces drastically. Patients state that they feel they can once again “catch their breath.” Mucous secretion is reduced.
Expiratory parameters increases from 20% to 39% (nearly double) of the predicted values.
FEV1/FVC ratio dropped from an average 45% before the procedure to 28% at 2 years follow up. This decline occurred due to maintenance of the FEV1 and an increase in the FVC.